The Science of COVID-19
This transmission electron microscope image shows SARS-CoV-2—the virus that causes COVID-19—isolated from a patient in the U.S. Coronaviruses are named for the "crown" of spikes on the virus particle's surface, which help the virus attach to cells and infect them.
Courtesy of NIAID/Flickr
Courtesy of NIAID/Flickr
How does an infectious disease like COVID-19 emerge?
Understanding the COVID-19 pandemic requires exploring the natural history of the novel coronavirus, called SARS-CoV-2, that causes it—where and how it lives, how it mutates and evolves, and how it interacts with humans—as well as how different peoples worldwide view and respond to it.
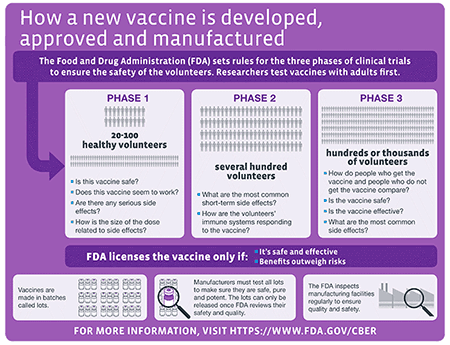
With dozens of COVID-19 vaccinations in development and some approved for use in record time, it is also important to understand how vaccines work, how they are developed and tested, and why vaccination is critical in the fight against COVID-19.

Fast Facts About the Novel Coronavirus SARS-CoV-2
For public health information about COVID-19, please visit Centers for Disease Control and Prevention. For Museum updates and polices, please visit our Health and Safety page.

COVID-19 and Related Research at the American Museum of Natural History
- Curator Nancy Simmons, curator-in-charge in the Department of Mammalogy and professor at the Museum's Richard Gilder Graduate School, is an evolutionary biologist researching bat biology, ecology, evolution, and conservation. She is part of a group using modeling methods to predict unrecognized wildlife host species for viruses related to SARS-CoV-2 that will help prioritize future sampling for emerging viruses and a member of the Natural Science Collections COVID-19 task force, a group that seeks to organize and make available data from natural history collections and publications for COVID-19 related research. This work, a collaboration with Consortium of European Taxonomic Facilities (CETAF) and Distributed System of Scientific Collections (DiSSCo), will allow for better documentation of relationships between wildlife hosts and their pathogens. Dr. Simmons is also a member of iDigBio’s ViralMuse Task Force, a group that seeks to develop more integrated, longer-term relationships between the virology research community and the natural history museums housing specimens relevant to understanding emerging pathogens. She is also engaged in bat conservation programs worldwide and has published on the threats to bats posed by COVID-19 and by misunderstandings about the role of bats in the current pandemic.
- Curator Ward Wheeler, curator in the Division of Invertebrate Zoology and professor at the Museum's Richard Gilder Graduate School, oversees and maintains the Museum's computation cluster, which is now a top provider of computational services for COVID-19 research.
- Senior Bioinformaticist Apurva Narechania is developing a project to study the early genomic epidemiology, transmission patterns, and molecular evolution of SARS-CoV-2, the virus that causes COVID-19, with the goal of informing important disease control and treatment insights. The proposed research is in collaboration with the Hackensack Meridian Health (HMH) network and the Center for Discovery and Innovation (CDI).
- Gerstner Postdoctoral Fellow in Bioinformatics and Computational Biology Victor Sojo is developing an epidemiological model of the spread of COVID-19 and the impact on healthcare systems.
- Assistant Director of Genomic Operations Anthony Caragiulo, Lab Manager Lauren Audi, and Senior Bioinformaticist Apurva Narechania are proposing comparative genomic research of SARS-CoV-2 to investigate similarities between humans and wildlife hosts, specifically big cats drawing on wildlife samples in the Museum’s collection and blood samples from the infected Bronx Zoo tigers and lions.
- Bioinformatics Specialist Dean Bobo is researching genomic sequence similarities between SARS-CoV-2 and all other non-SARS virus genomes to examine how and when these arose and what they might mean.
- U.S. Department of Energy postdoctoral fellow Michael Tessler is using climate models to examine the virulence of SARS-CoV-2 in different geographic regions of the globe.
- Museum Research Associate Paul Planet, a physician and researcher at Children’s Hospital of Philadelphia (CHoP), has developed a novel sequence-typing technique for SARS-CoV-2 typing. His work has revealed multiple waves of SARS CoV-2 spread and can be viewed on GitHub.
- Visiting Scientist Chase Nelson, a former Gerstner Scholar in Bioinformatics and Computational Biology at the Museum, and colleagues have identified a new gene in SARS-CoV-2 that may have contributed to its unique biology and pandemic potential.